2026 | Volume 27 | Issue 1
I want to speak directly to an issue that has understandably been generating some debate within our surgical community: the proposal by the Australian Orthopaedic Association and the New Zealand Orthopaedic Association to pursue direct accreditation and establish a separate orthopaedic college.
I am not an orthopaedic surgeon, but I care deeply about this issue and believe our profession is stronger when the nine specialties remain within a single, united College.
I would be very sorry to see our orthopaedic colleagues leave RACS. Not only because of what they contribute, but because separation is an irreversible step, with stated outcomes (cost savings, specialty leadership, modernised training environment) that I am confident can be better achieved through reform within the existing framework underpinned by unity.
Change delivered now
A central argument being made for leaving RACS relates to training fees. It is true that training fees have risen over recent years. Like every organisation, we have faced post-COVID-19 inflation and rising operating costs, and most surgical specialties have had to increase fees as well.
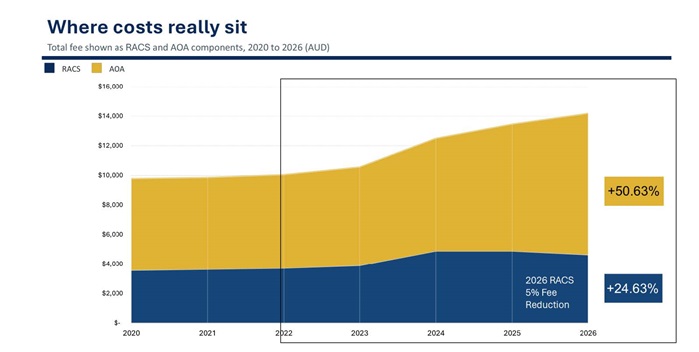
What is also true is that over the past two years RACS has restored financial discipline and governance. We have regained financial soundness, strengthened fiscal oversight, and undertaken significant cost efficiencies including IT reform delivering more than $1 million in savings, procurement savings, and structural changes that are already bearing fruit.
With the groundwork laid, we have been able to freeze member fees for the past two years, deliver a five per cent reduction in the RACS component of training fees in 2026, and reduce skill course costs. With further reforms underway, we believe that reductions of up to 30 per cent are achievable within the current training framework.
This is the context for the Surgical Pathways Strategy and RACS’ proposal for a modernised, faculty-based model within the College. This approach strengthens specialty leadership while preserving unity; modernises training while safeguarding quality and patient safety; improves access, diversity and equitable regional distribution of training posts; and reduces cost and duplication without creating additional organisational layers. It delivers genuine reform without the financial, structural and regulatory risks inherent in establishing a separate college.
Training is a team sport …
I also want to address the claim that “the specialties do all the work” when it comes to training. Training is delivered primarily in hospitals by supervisors and trainers—people who are members of both RACS and their specialty societies. Under current arrangements, RACS engages AOA to deliver 16 of 41 activities through a service agreement.
While technical training is delivered outside RACS, the College provides important elements that go into making you a surgeon: accreditation, governance, examinations, professional standards, legal frameworks, education programs and independent oversight. These are collective functions that require scale, infrastructure and regulatory credibility.
… and it’s only one part of what our College does
Some have criticised RACS for having more than 100 committees. We make no apology for this. RACS is a broad church, representing the many and varied interests of Fellows and Trainees across specialties, states and territories, and Aotearoa New Zealand. Our committees are how members are heard, represented and engaged.
RACS directly supports its members through education, research and scholarships, and provides inclusive national structures that bring together rural and regional surgeons, Aboriginal, Torres Strait Island and Māori surgeons, and those working in academic, military and medico-legal practice. Shared services, including professional standards, the RACS Library, Foundation scholarships, wellbeing programs and global health, benefit us all.
![]()
Strong, unified, trusted
Let me be clear: specialty societies play an essential role in our career as surgeons. But with more than 50 specialty and subspecialty societies now operating across our region, surgery is becoming increasingly fragmented. That makes a unifying College, with the scale to cut through and represent all interests, more important than ever.
This is a pivotal moment. My strong view is that we are stronger together, and that the future of surgical training, standards and advocacy is best served by reform within a united RACS.
If you value a strong surgical voice, collegiality, international recognition, professional development and effective advocacy, then a unified RACS remains our best foundation. Fragmentation may promise short-term gains, but it carries long-term consequences for all specialties.
Thank you for engaging thoughtfully in this conversation and for your continued commitment to the profession.
Keen to learn more?
• Read RACS position on AOA/NZOA proposed split
• View the recording and slide presentation from our 29 January webinar for Australian orthopaedic members.
• Review our updated FAQs which address the questions raised at the webinar and many more.
• For questions or further discussion, contact me at [email protected].
• Review previous communications and resources on this topic, using your RACS login.
Warm regards,
Professor Owen Ung
President